Skip to content
972-872-8408
[email protected]
HOME
About Us
Dr. Oliver Ghalambor
Dr. Aboul-Fettouh
Conditions
ACL (Anterior Cruciate Ligament) Injuries
Anatomy of the Spine
Biceps Tendonitis
Bursitis of the Hip
Cervical Radiculopathy
Cluster Headaches
Coccydynia
Complex Regional Pain Syndrome
Degenerative Disc Disease
Facet Joint Syndrome
Frozen Shoulder Adhesive Capsuliti
Glenoid Labrum Tear
Herniated Disc
Herniated Disc Cervical
Iliotibial Band Syndrome
Inflammatory Arthritis of the Hip
Lateral Epicondylitis Tennis Elbow
Lumbar Radiculopathy Sciatica
Long Covid SARS-CoV-2
Long Covid Assessment Test
Meniscus Tears
Migraine Headaches
Occipital Neuralgia
Osteoarthritis of the Hip
Osteoarthritis of the Knee
Osteoarthritis of the Shoulder
Piriformis Syndrome
Plantar Fasciitis
Post Laminectomy Syndrome
Post Whiplash Headache
Rotator Cuff Injuries
Sacroiliac Joint Pain
Shoulder Impingement Syndrome
Spondylosis
Suprascapular Neuropathy
Whiplash
Treatments
BOTOX®injections for chronic migraine
Back Pain
Lower Back Pain
Caudal Epidural Steroid Injection
Cervical Epidural Steroid Injection
Cervical Facet Radio-frequency Neurotomy
Facet Joint Injections
Foot and Ankle Pain Doctor
Genicular Nerve Ablation (RF Neurotomy)
genicular nerve block (G Block)
Hip Pain Doctor
(HYALGAN) injection for knee pain
intraoperative monitoring of the nerves
Knee Pain
Long Covid Treatment
Long Covid Assessment Test
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural Steroid
Manipulation Under Anesthesia (MUA)
Medial Branch Block (Lumbar)
medial branch block (Cervical)
PRP therapy (Overview)
PRP therapy for chronic back pain
PRP therapy chronic knee Pain
PRP Therapy for Hip Arthritis
PRP Therapy for Shoulder Pain
radiofrequency neurotomy Lumbar Facet
radiofrequency neurotomy thoracic Facet
Sacroiliac Joint Steroid Injection
Shoulder Pain
Shoulder Pain Doctor
sphenopalatine ganglion (SPG) block
spinal cord stimulator (Trial)
Spinal Cord Stimulator Implant
Stellate Ganglion Block
Subacromial Injection
Suprascapular Nerve Block
Trigger Point Injection
Viscosupplementation for Arthritis
YESS selective endoscopic discectomy
REGENERATIVE
Bone Marrow Stem Cells
Platelet Rich Plasma (PRP)
STEM CELLS
Regenerative Medicine
Reviews
Contact
HOME
About Us
Dr. Oliver Ghalambor
Dr. Aboul-Fettouh
Conditions
ACL (Anterior Cruciate Ligament) Injuries
Anatomy of the Spine
Biceps Tendonitis
Bursitis of the Hip
Cervical Radiculopathy
Cluster Headaches
Coccydynia
Complex Regional Pain Syndrome
Degenerative Disc Disease
Facet Joint Syndrome
Frozen Shoulder Adhesive Capsuliti
Glenoid Labrum Tear
Herniated Disc
Herniated Disc Cervical
Iliotibial Band Syndrome
Inflammatory Arthritis of the Hip
Lateral Epicondylitis Tennis Elbow
Lumbar Radiculopathy Sciatica
Long Covid SARS-CoV-2
Long Covid Assessment Test
Meniscus Tears
Migraine Headaches
Occipital Neuralgia
Osteoarthritis of the Hip
Osteoarthritis of the Knee
Osteoarthritis of the Shoulder
Piriformis Syndrome
Plantar Fasciitis
Post Laminectomy Syndrome
Post Whiplash Headache
Rotator Cuff Injuries
Sacroiliac Joint Pain
Shoulder Impingement Syndrome
Spondylosis
Suprascapular Neuropathy
Whiplash
Treatments
BOTOX®injections for chronic migraine
Back Pain
Lower Back Pain
Caudal Epidural Steroid Injection
Cervical Epidural Steroid Injection
Cervical Facet Radio-frequency Neurotomy
Facet Joint Injections
Foot and Ankle Pain Doctor
Genicular Nerve Ablation (RF Neurotomy)
genicular nerve block (G Block)
Hip Pain Doctor
(HYALGAN) injection for knee pain
intraoperative monitoring of the nerves
Knee Pain
Long Covid Treatment
Long Covid Assessment Test
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural Steroid
Manipulation Under Anesthesia (MUA)
Medial Branch Block (Lumbar)
medial branch block (Cervical)
PRP therapy (Overview)
PRP therapy for chronic back pain
PRP therapy chronic knee Pain
PRP Therapy for Hip Arthritis
PRP Therapy for Shoulder Pain
radiofrequency neurotomy Lumbar Facet
radiofrequency neurotomy thoracic Facet
Sacroiliac Joint Steroid Injection
Shoulder Pain
Shoulder Pain Doctor
sphenopalatine ganglion (SPG) block
spinal cord stimulator (Trial)
Spinal Cord Stimulator Implant
Stellate Ganglion Block
Subacromial Injection
Suprascapular Nerve Block
Trigger Point Injection
Viscosupplementation for Arthritis
YESS selective endoscopic discectomy
REGENERATIVE
Bone Marrow Stem Cells
Platelet Rich Plasma (PRP)
STEM CELLS
Regenerative Medicine
Reviews
Contact
Locations
Allen
Coppell
Fort Worth
Garland
Corporate Wellness
Case Series
Spine and Pain Case Studies 1
Chiropractic Pain Case Studies 4
Chiropractic Pain Case Studies 3
Chiropractic Pain Case Studies 2
Chiropractic Pain Case Studies 1
Pain Management 101 Case Series
Blog
Locations
Allen
Coppell
Fort Worth
Garland
Corporate Wellness
Case Series
Spine and Pain Case Studies 1
Chiropractic Pain Case Studies 4
Chiropractic Pain Case Studies 3
Chiropractic Pain Case Studies 2
Chiropractic Pain Case Studies 1
Pain Management 101 Case Series
Blog
Home
About Us
Corporate Wellness Program
Blog
Locations
Allen
Coppell
Fort Worth
Garland
Conditions
Anatomy of the Spine
Biceps Tendonitis
Bursitis of the Hip
Cervical Radiculopathy
Cluster Headaches
Coccydynia
Complex Regional Pain Syndrome
Degenerative Disc Disease
Facet Joint Syndrome
Frozen Shoulder Adhesive Capsuliti
Glenoid Labrum Tear
Herniated Disc
Herniated Disc Cervical
Iliotibial Band Syndrome
Inflammatory Arthritis of the Hip
Lateral Epicondylitis Tennis Elbow
Lumbar Radiculopathy Sciatica
Migraine Headaches
Occipital Neuralgia
Osteoarthritis of the Hip
Osteoarthritis of the Knee
Osteoarthritis of the Shoulder
Piriformis Syndrome
Plantar Fasciitis
Post Laminectomy Syndrome
Post Whiplash Headache
Rotator Cuff Injuries
Sacroiliac Joint Pain
Shoulder Impingement Syndrome
Spondylosis
Suprascapular Neuropathy
Whiplash
Treatments
Back Pain
Lower Back Pain
Botox Injections Chronic Migraine
Caudal Epidural Steroid Injection
Cervical Epidural Steroid
Cervical Facet Radiofrequency
Facet Joint Injections
Foot and Ankle Pain Doctor
Genicular Nerve Ablation
Genicular Nerve Block G Block
Hip Pain Doctor
Hyalgan Injection for Knee Pain
Intraoperative Monitoring Nerves
Knee Pain Doctor
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural
Manipulation Under Anesthesia
Medial Branch Block
Medial Branch Block Cervical
PRP Therapy for Hip Arthritis
PRP Therapy for Shoulder Pain
PRP Therapy Overview
Radiofrequency Neurotomy Lumba
Radiofrequency Neurotomy Thoracic
Sacroiliac Joint Steroid Injection
Shoulder Pain
Shoulder Pain Doctor
Sphenopalatine Ganglion Block
Spinal Cord Stimulator Implant
Spinal Cord Stimulator Trial
Stellate Ganglion Block
Trigger Point Injection
Viscosupplementation for Arthritis
Selective Endoscopic Discectom
Regenerative Medicine
Bone Marrow Stem Cells
Plasma Rich Protein
Regenerative Medicine
Case Series
Spine and Pain Case Studies 1
Chiropractic Pain Case Studies 4
Chiropractic Pain Case Studies 3
Chiropractic Pain Case Studies 2
Chiropractic Pain Case Studies 1
Pain Management 101 Case Series
Contact
Home
About Us
Corporate Wellness Program
Blog
Locations
Allen
Coppell
Fort Worth
Garland
Conditions
Anatomy of the Spine
Biceps Tendonitis
Bursitis of the Hip
Cervical Radiculopathy
Cluster Headaches
Coccydynia
Complex Regional Pain Syndrome
Degenerative Disc Disease
Facet Joint Syndrome
Frozen Shoulder Adhesive Capsuliti
Glenoid Labrum Tear
Herniated Disc
Herniated Disc Cervical
Iliotibial Band Syndrome
Inflammatory Arthritis of the Hip
Lateral Epicondylitis Tennis Elbow
Lumbar Radiculopathy Sciatica
Migraine Headaches
Occipital Neuralgia
Osteoarthritis of the Hip
Osteoarthritis of the Knee
Osteoarthritis of the Shoulder
Piriformis Syndrome
Plantar Fasciitis
Post Laminectomy Syndrome
Post Whiplash Headache
Rotator Cuff Injuries
Sacroiliac Joint Pain
Shoulder Impingement Syndrome
Spondylosis
Suprascapular Neuropathy
Whiplash
Treatments
Back Pain
Lower Back Pain
Botox Injections Chronic Migraine
Caudal Epidural Steroid Injection
Cervical Epidural Steroid
Cervical Facet Radiofrequency
Facet Joint Injections
Foot and Ankle Pain Doctor
Genicular Nerve Ablation
Genicular Nerve Block G Block
Hip Pain Doctor
Hyalgan Injection for Knee Pain
Intraoperative Monitoring Nerves
Knee Pain Doctor
Lumbar Sympathetic Block
Lumbar Transforaminal Epidural
Manipulation Under Anesthesia
Medial Branch Block
Medial Branch Block Cervical
PRP Therapy for Hip Arthritis
PRP Therapy for Shoulder Pain
PRP Therapy Overview
Radiofrequency Neurotomy Lumba
Radiofrequency Neurotomy Thoracic
Sacroiliac Joint Steroid Injection
Shoulder Pain
Shoulder Pain Doctor
Sphenopalatine Ganglion Block
Spinal Cord Stimulator Implant
Spinal Cord Stimulator Trial
Stellate Ganglion Block
Trigger Point Injection
Viscosupplementation for Arthritis
Selective Endoscopic Discectom
Regenerative Medicine
Bone Marrow Stem Cells
Plasma Rich Protein
Regenerative Medicine
Case Series
Spine and Pain Case Studies 1
Chiropractic Pain Case Studies 4
Chiropractic Pain Case Studies 3
Chiropractic Pain Case Studies 2
Chiropractic Pain Case Studies 1
Pain Management 101 Case Series
Contact
Chiropractic & Pain Case Studies
Oliver Ghalambor, MD, DABA, FIPP, DABIPP, DABPM
Case 4
Case 4 Details
52 year old female
Referred by her PCP
Chief Complaint “Right Low Back and leg Pain”
Seen in consultation on 03/03/2017
Reported pain being there on and off for about a couple of years
Gradual recent worsening in the last couple months
No known trigger event.
Tried OTC NSAIDs, Massage, Acupuncture, Physical Therapy, Heating Pad, muscle relaxant (Flexeril)
Patient initially had relief from chiropractic care, but last couple treatments made her “worse” so she stopped going to her chiropractor
Patient has past medical history of cervical spine fusion (C5-6 ACDF).
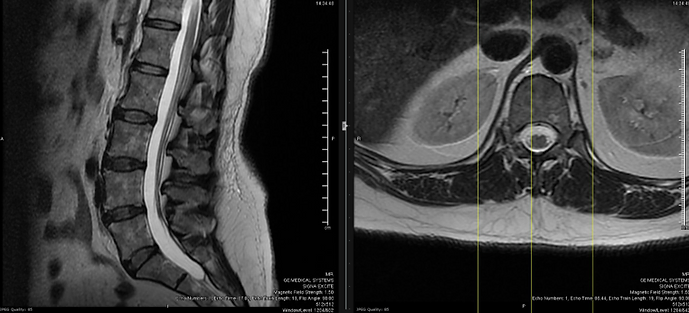
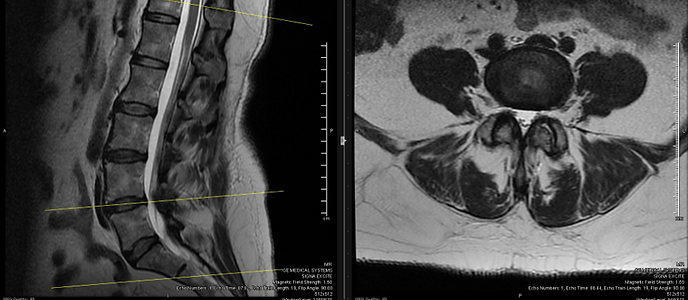
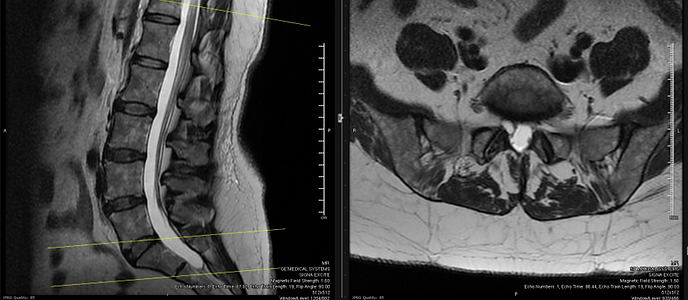
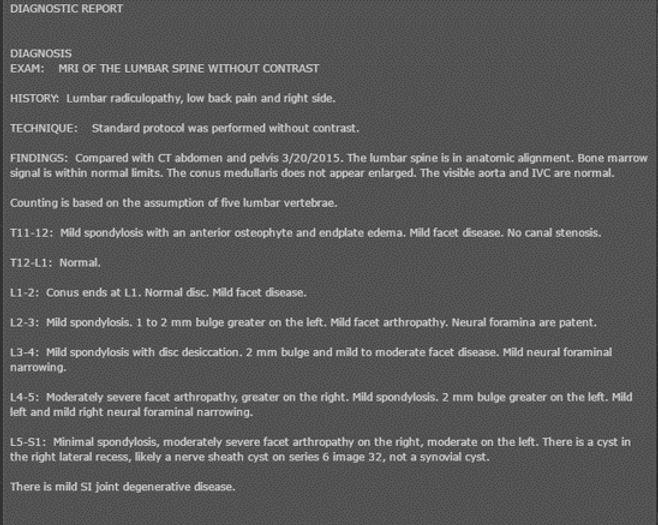
After initial consultation with her PCP, MRI of the Lumbar spine was ordered and was “abnormal”.
The PCP recommended referral to a spine surgeon first. She express her desire to “try everything else first” and so she was referred to us.
Pain was described as “constant”, “continuous”, “numbing” and ”radiating down the leg”
Pain was rated average 6/10 VAS, max 9/10 VAS
Upon exam she was in no apparent distress upon rest
Tenderness present over the right low lumbar region
Facet loading maneuvers positive on the right
Straight leg raise test positive on the right
Motor exam normal, sensory suggestive of numbness to light touch and cold temperature in the right S1 dermatome
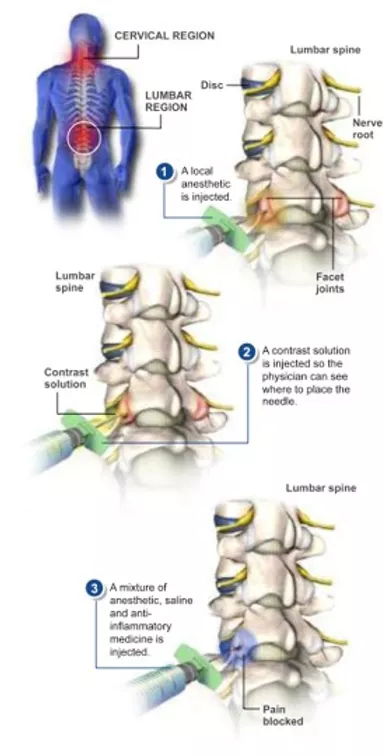
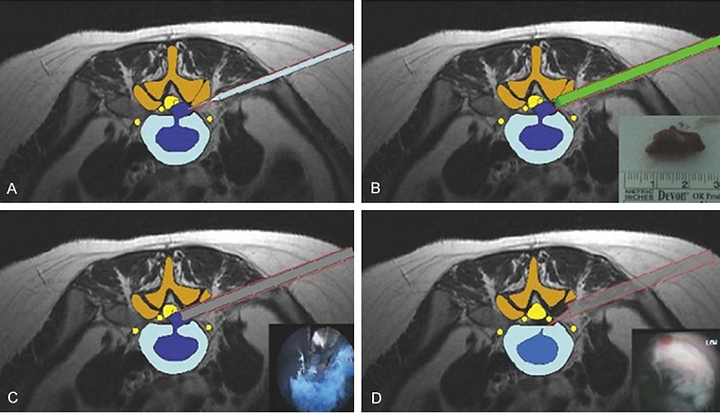
Facet Joint Injection
On 03/07/2017 the patient underwent:
1. Right L5/S1 facet aspiration and injection with steroids
2. Right L5 and S1 transforaminal epidural steroid injection
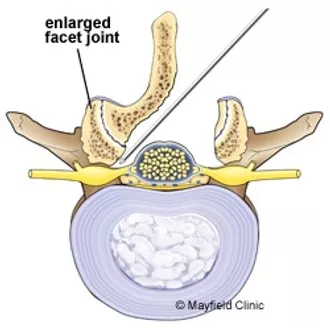
Can mobilizing a facet joint that has arthritis and an adjacent facet cyst temporarily irritate a nerve root?
It depends
Was it the case here?
It depends
What if the patient does not get good and/or sustained relief from combination if epidural steroid injections and facet injections?
It depends
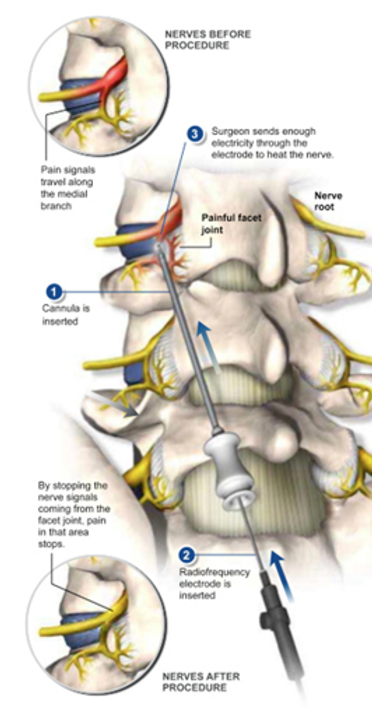
Lumbar Radiofrequency Neurotomy (Rhizotomy)
Right low back pain only which responds short term to the lumbar facet injections
Lumbar facet joint medial branch RFA
Lumbar radiculopathy which does not respond to combination of facet cyst injections and epidural steroid injections
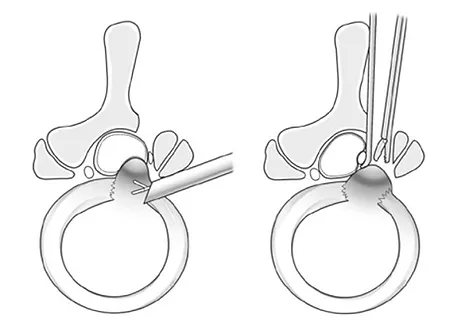
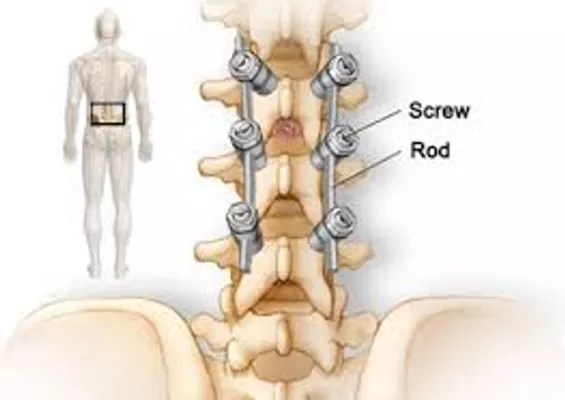
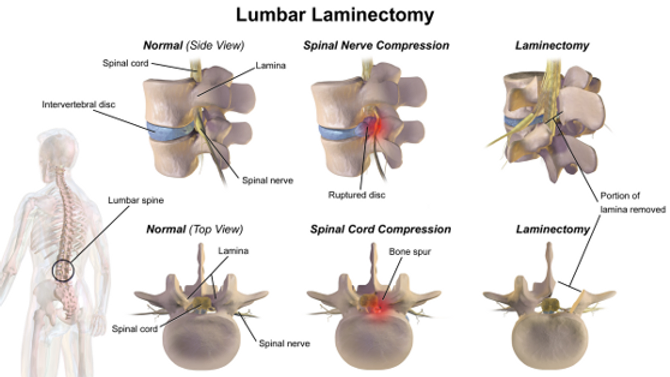
Old fashion way:
Lumbar laminectomy, facetectomy